Contraceptive Access and State Telehealth Policies

Across the United States, the COVID-19 pandemic has greatly expanded the use of telehealth. Many states expanded telehealth access and coverage during the pandemic to allow access to medical care while reducing people’s exposure to COVID-19. Currently, many of these additional policies are set to expire at the end of the federal public health emergency (currently extended through the end of 2021), although some states are moving to make certain changes permanent. Our own polling data found that 77% of respondents agree that telehealth is a useful method to get birth control when in-person visits are not possible.
To better understand the ways in which telehealth access has changed and expanded over the course of the pandemic, we have created two new ways to visualize the state-level landscape of telehealth access for Medicaid and private payor insurance both pre-COVID and during the pandemic.
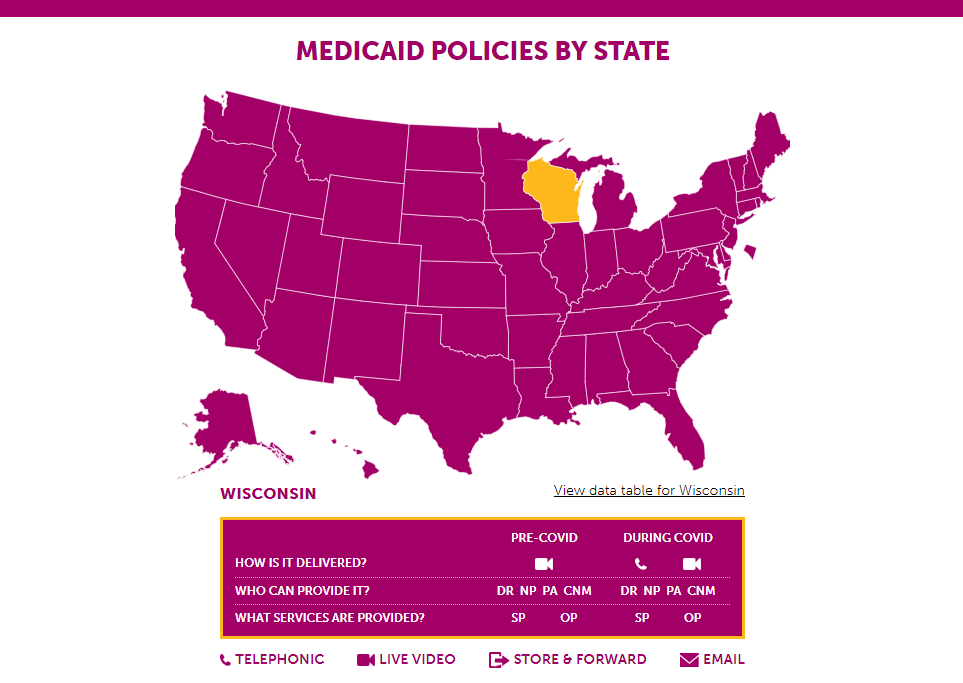
In the first, we have built maps that, when a specific state is selected, show high-level information which answers three questions: how is it delivered? Who can provide it? And what services are provided?
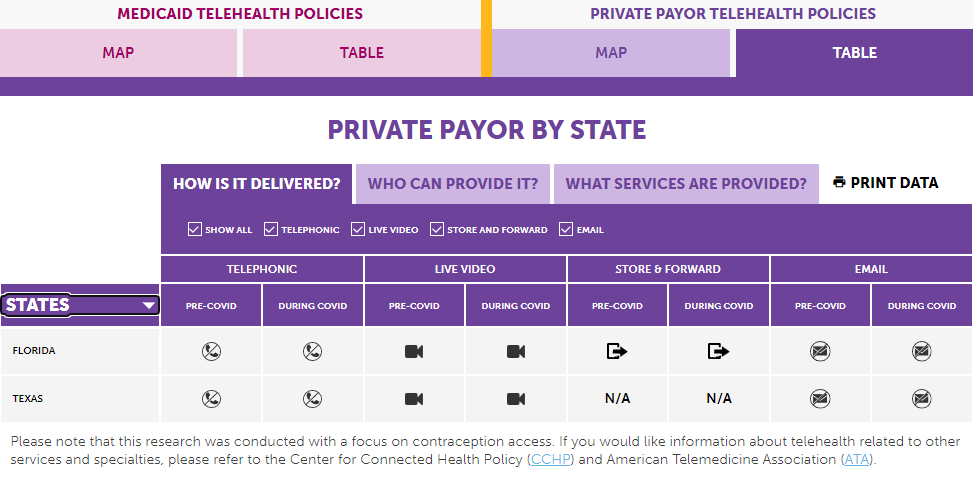
In the second, we have created interactive tables answering these same questions with more detail that allow users to compare data from pre-COVID and during COVID both within and between states.
Why these three questions?
Overall, we’ve chosen these three questions to help to simplify complicated policies so that advocates, public health officials, elected officials, and everyday health care users can more easily understand the various telehealth policies that are most likely to affect access to birth control in their states.
How is it delivered?
Providers and patients can communicate in multiple ways beyond in-person visits, all of which are potential telehealth delivery methods. Our telehealth information includes four options: telephonic, or the use of a standard phone call to have a telehealth appointment; live video, a two-way audio-video call between a patient and provider ; store and forward, which is the collection and temporary storage of medical data that is later forwarded through a secure online system to a secondary site for evaluation; and email, or the use of solely email-based communication between provider and patient.
Who can provide it?
There are multiple types of providers who are eligible to provide telehealth however, we focus on the four that are often involved in providing contraception: physicians, nurse practitioners, physician assistants, and nurse-midwives.
What services are provided?
Since most policies pertaining to telehealth as a practice do not include specific language on services related to contraception, we looked for language specifically about service parity (meaning that any services covered for patients in-person must also be covered for patients when delivered via telehealth) and online prescribing (which is different than an electronic prescription and refers to the act of prescribing drugs based on an online interaction).
What trends do we see in this data?
A number of points stand out when looking at the data presented under each of the three questions we ask.
- Medicaid policies, which are more specific as to what is required to be covered, are more expansive than private payor policies, many of which allow coverage of certain telehealth delivery methods, but do not require it.
- The number of states allowing telehealth to by phone for those covered by Medicaid has increased significantly during the Coronavirus pandemic. Prior to COVID only two states covered it, while currently 49 states and DC do.
- During COVID, about 90% of states and DC require service parity under Medicaid and three-quarters require it under private payor insurance. This has increased from about two-thirds of states pre-COVID for both Medicaid and private payor.
- Under Medicaid, about two-thirds of states allowed online prescribing without a prior provider-patient relationship, while about one-sixth do require a prior provider-patient relationship. Neither figure has changed since the start of the pandemic.
- Under private insurance however, the number of states allowing online prescribing with no prior provider-patient relationship increased from 26 pre-COVID to 32 during COVID. The number of states requiring a prior provider-patient relationship increased from seven to ten.
What is the future of telehealth?
We have seen telehealth’s potential in increasing access to health care, including birth control. However, it is not without potential drawbacks. Our polling data showed that of those with annual household incomes under $50,000 only 21% of respondents reported understanding telehealth, compared to 67% of those with annual household incomes over $50,000. This knowledge gap for people with lower incomes could greatly curtail their telehealth usage.
Other issues that require thought to address include concerns over quality of care, payment parity, HIPAA compliance, individual privacy, and internet and technology access. Ultimately, all these issues need addressing to ensure that telehealth is not only beneficial but also equitable.
Samantha Berg earned her Master of Public Health and a Certificate in Sexuality, Sexual and Reproductive Health from Columbia University Mailman School of Public Health in May 2020. As the Policy Fellow for PTD, Sam works on state policy and telehealth access, which align nicely with her passion for public health and reproductive justice.


